




Laparoscopic Right Hemicolectomy with Intracorporeal Anastomosis
January 4, 2012
Graziano Pernazza (Rome – Italy)
Summary: Laparoscopic right colic resection for malignancy has been demonstrated to be safe and reproducible and is nowadays widely accepted. Laparoscopic right colectomy is considered one of the most difficult minimally invasive colorectal procedures, more difficult than open colectomy. The video shows a totally laparoscopic right colectomy. All the steps of the procedure are completed through the minimally invasive technique. This is considered the most beneficial approach with less postoperative pain, short-term postoperative ileus, earlier return to daily activity and better choice for the minilaparotomy (usually supra-pubic).
The procedure is carried out using four trocarts. The first one, placed with an open technique, is inserted on the left pararectal line, just above the transverse umbilical line. Two operative ports are placed on the same line in the left hypochondrion and in the left iliac fussa. One ancillary port, used to retract the cecum or the transverse colon during the different steps of the procedure, is placed in the right iliac fussa. The operative table is placed in a slight reverse Trendelenburg and tilted laterally to the left.
Main surgeon and assistant surgeon stay on the patient left side.
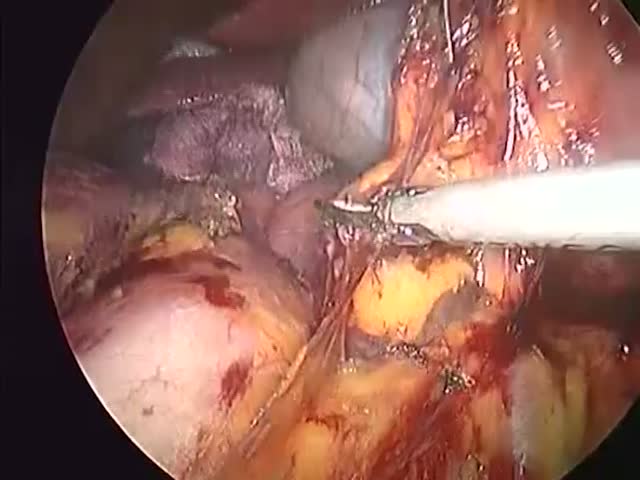
The first step of the procedure is the identification of the lateral margin of the superior mesenteric vein. This step is made easier applying a gentle traction on the cecum, which allows to identify the route of the ileocolic vessels. This way the lymphadenectomy is performed along the mesenteric route in a caudo-cranial shape, thus identifying the ileocolic vessels, the right (inconstant) vessels and the lateral aspect of the origin of the middle colic vessels to reach their right branch.
We consider this part of the procedure the most important and difficult one. It is fundamental to stay on the right plane, to correctly identify the structures (the duodenum, the head of the pancreas…) and to keep clean the operative field. An effective cohoperation of the assistant surgeon in retracting and exposing the operative field is crucial.
Once completed this step, before to begin the gastroepiploic lymphadenectomy, when it is indicated, the transverse colon is transected and fully mobilized. The last ileal loop is transected as well and an intracorporeal side-to-side, iso-peristaltic ileo-colic anastomosis is fashioned with an endoscopic linear stapler. The viscerotomy is closed by a double-layer running suture.
In our experience this is the is the routinely adopted technique for laparoscopic right colic resections.
