




Chicago 2009 Video – Robotic Total Mesorectal Excision for Rectal Cancer. Technical Aspects
January 20, 2010
Paolo Pietro Bianchi (Grosseto – Italy)
SUMMARY
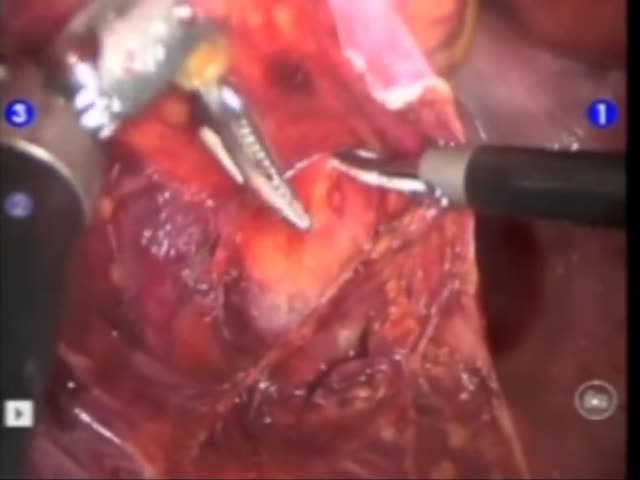
The video shows technical aspects of robotic Total Mesorectal Excision (TME). Three robotic and two laparoscopic trocars were inserted. The cart and the arms of Da Vinci© are maintained in the same position during all the operation and the technique is full robotic. The anastomosis is performed under laparoscopic guidance with the Knight-Griffen technique.
Background/Hypothesis
The video shows technical aspects of robotic total mesorectal excision (TME) in rectal cancer
Materials & Methods
The Robotic system used was a four arms Da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA, USA). Three 8 mm robotic and two 12 mm laparoscopic trocars were inserted. After a laparoscopic exploration of the abdominal cavity the robot is connected. The cart and the arms of Da Vinci© are maintained in the same position during all the operation, sometimesthe assistant changes the angle of the robotic arm, just moving the trocars, without detachment of the robot. The first step is splenic flexure mobilization along the posterior plane covered by Toldt’s fascia, with a posterior dissection of the transverse mesocolon. The inferior mesenteric vessels are then divided with laparoscopic clips positioned by the assistant. Sigmoid and descending colon are mobilized with a medial to lateral approach. Then rectal dissection proceeds into the pelvis and the TME is performed. The robot is disengaged and the distal rectal division is completed laparoscopically with an EndoGIA and the anastomosis is performed under laparoscopic guidance with the Knight-Griffen technique. A loop laparoscopic ileostomy is
done when the anastomosis is performed at less then 5 cm from the anal verge
Results
From August 2008 to June 2009 27 patients with cancer of the middle and lower rectum were treated with a robotic TME. In 5 cases (18.5%) a laparoscopic mobilization of the splenic flexure was performed and the robot was connected for vascular dissection and TME, in the other 22 patients (81.5%) a full robotic operation was made. Mean operative time was 258.2 minutes.
Conclusions
Robotic anterior resection in rectal cancer is a safe and feasible operation. The learning curve for an expert laparoscopic surgeon seems to be shorter than for the same laparoscopic procedure.
