




Chicago 2009 Video – Robotic-Assisted Trans-Hital Total Esophagectomy: a Two-Year Single Center Experience
January 13, 2010
K. Kosari, D. H. Dunn
Background/Hypothesis
Minimally Invasive Esophagectomy has emerged as an important procedure for disease management in esophageal cancer (EC) with lymph node retrieval, clear margin status, lower leak rate as well as less morbidity and shorter hospital stays comparable to open procedures. In this report we describe our experience with trans-hiatal robotic esophagectomy (RE).
Materials & Methods
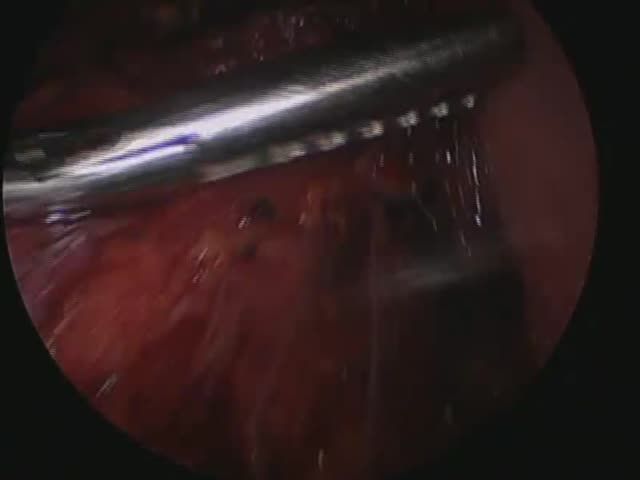
From March 2007 to June 2009, 36 patients eligible for RE were evaluated by a multidisciplinary team in accordance with NCCN guidelines, following which, surgery (with or without neoadjuvant therapy) were planned. The RE procedure involved laparoscopic mobilization of the stomach from the gastroesophageal junction to the pylorus followed by a celiac lymph node resection. The robot was then used for mediastinal esophageal dissection. A gastric tube was created, brought up into the neck, and a 25 mm EEA stapled anastomosis was performed.
Results
Of 36 patients undergoing RE, 1 patient had an extensive benign stricture, 1 had high grade dysplasia and 34 had EC. Fourteen patients received neoadjuvant chemoradiation and 2 neoadjuvant chemotherapy only. Four patients were converted from robotic to open. Median operative time was 311 minutes (range, 226 to 491). Mean number of lymph nodes removed was 18 and estimated blood loss was 97.2 ml. Eleven patients had an ICU stay of <24 hrs; 15 had 1-2 days and 10 had 2-21 days of ICU stay. Median length of hospital stay was 9 days (range, 6 to 36). Overall leak rate was 22.2% (8/36). Recurrent nerve injury was noted in 27.8% (10/36) patients, and operative mortality was 2.8% (1/36).
Conclusions
RE is a safe oncologic operation for EC. The benefits include complete mediastinal dissection without thoracoscopy and satisfactory lymph node retrieval. Broader use of the technology in the setting of comprehensive esophageal cancer programs is recommended.
