




Laparoscopic Splenectomy
December 27, 2011
Graziano Pernazza (Rome – Italy)
Summary: Laparoscopic splenectomy has gained universal acceptance and today it is probably regarded as a Gold standard in removal of benign and normal sized spleens. Despite this, splenectomy surgery has always been considered burdened by high morbidity and mortality and potentially serious bleeding.
The routine application of laparoscopy in case of thalassemia major is controversial, however, for the increased bleeding risk. The splenic volume and vascular hilum and shape can be limiting factors. The prevention of postoperative complications, mainly thrombotic and septic, of intervention and the characteristics of patients, is usually entrusted to the scrupulous implementation of pre-and postoperative care protocols.
The video presents the technique we are routinely adopting. The video refers to the case of a 35-year-old female patient, suffering from symptomatic fast-growing cystic lesion of the spleen (lymphangioma). The patient is usually placed in a supine position on the operating table, with legs abductees, a slight anti-Trendelenburg position and rotated approximately 15° to the right. The operator is positioned between the legs of the patient, the attendants on the right side. We usually use four ports: pararectal on the transverse umbilical line is for the 30 ° lens, the main operative ones 4 cm upwards on the median umbilical line and on the left side, and an accessory port is placed in the right upper quadrant.
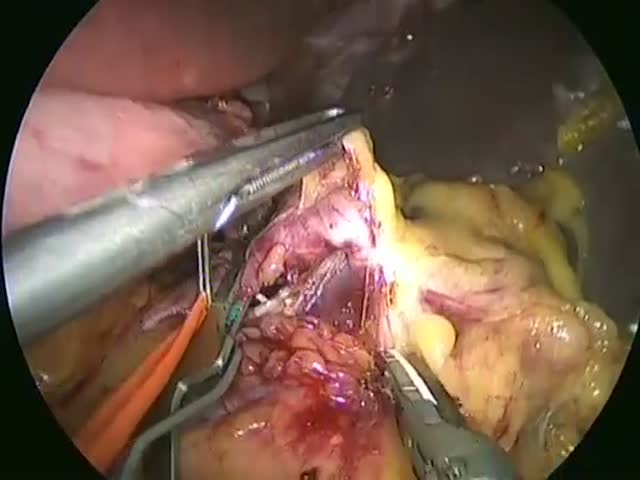
An accurate preoperative CT-scan study with tridimensional reconstruction is useful to detect size and volume of the spleen and, moreover, to understand the conformation of the vascular hilum. The video illustrates the surgical steps in succession: 1) section of the gastrocolic ligament and short gastric vessels, 2) isolation of the splenic artery above the upper edge of the panceas and clamping (this maneuver increases the safety of the vascular dissection and causes a reduction in volume of the spleen), 3) section of the splenic artery downstream of the last pancreatic branch immediately before the main hilar branches , 4) preparation and section of the splenic vein, 5) complete mobilization of the spleen. The extraction of the piece, previously inserted into a bag may be performed by a small suprapubic incision.
The more hemorragic step of the procedure is the dissection of the splenic hilum. We perform a systematic preventive clamping of the splenic artery. This allow to carry out a careful and safe dissection of the splenic artery and can also be helpful to identify and preserve all the small arterial branches directed to the pancreatic tail.
