




Hyrtl artery preservation during robotic distal gastric resection and D2 lymphadenectomy.
July 2, 2012
Graziano Pernazza (Rome – Italy)
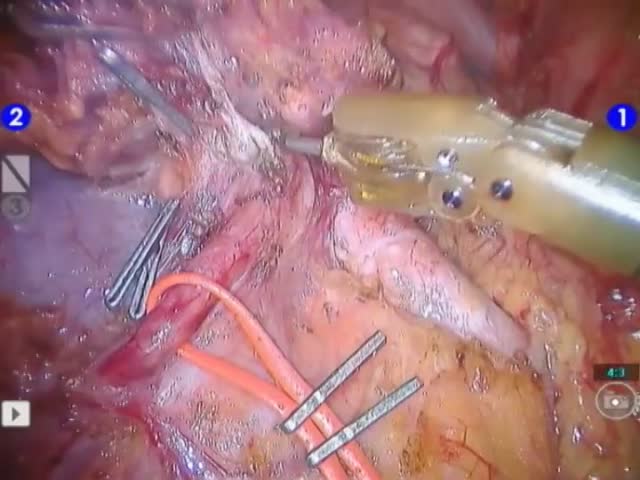
Age: 62 ASA score: 2 Previous Surgeries: no Histology (if any): gastric adenocarcinoma T2 N1 M0 History: Female patient 62yrs old, good general condition, sent to our attention by her physician, who had indicated an endoscopic study after the onset of a symptomatology characterized by postprandial abdominal pain, abdominal swelling, loss of appetite for flesh foods and mild anemia. The endoscopy revealed the presence of an excavated and ulcerated lesion, in the antral region. Biopsies were positive for adenocarcinoma. The total body CT scan was negative for distant lesions and suspicious lymphadenopathy. The vascular reconstruction, performed after the surgical procedure, confirmed the intraoperative finding of the accessory hepatic artery. Surgery Description: Induction of pneumoperitoneum with open technique One umbilical port for the endoscope, two robotic ports on right pararectal line and left flank. Two accessory ports on left pararectal line and right hypochondrion. The tumor is placed along the greater curvature of the stomach, not appearing to infiltrate the serosa. Absence of peritoneal carcinomatosis. No detectable liver lesions. No free fluid. The procedure is carried out with a full robotic approach. Coloepiploic detachment. Isolation and section of the right gastroepiploic vessels after infra-pyloric lymphadenectomy (4d ? 6). Isolation and section of the right gastric vessels and regional lymphadenectomy (5) Preparation of the duodenum and section with linear GIA stapler. Dissection of the hepato-duodenal ligament performing an en-bloc counterclockwise D2 lymphadenectomy along the branches of the common hepatic and proper hepatic artery, removing the periportal, celiac, left gastric, splenic and proximal gastric lymphnodes (12a, 8a, 9, 11p, 7) exposing the right diaphragmatic pillar. It is present a large caliber accessory left hepatic artery coming from the left gastric artery (Hyrtl?s artery), which is spared, performing the lymphadenectomy (1 and 3) along its main course, selectively closing and sectioning the gastric branches. Gastric section at the proximal third with linear GIA stapler.
