




Chicago 2009 Video – Robot-Assisted Major and Extended Hepatectomies
January 13, 2010
P. Addeo
SUMMARY
Major liver resections still represent a technical challenge for minimally invasive surgery. This presentation describes the intra and postoperative outcomes of one of the larger series of robotic major liver resections. The encouraging results obtained with the robotic approach for major liver resection in term of conversion rate, blood transfusion and postoperative morbidity confirm the feasibility and safety of the technique. Robotic represents a new technical option for performing minimally invasive major liver resections.
Background/Hypothesis
Laparoscopy is gaining widespread acceptance for liver resections. Most of the resections performed laparoscopically are minor or non anatomical resections, while a few of laparoscopic major hepatic resections have been reported until recently. The robotic technology due to some technical advantages could improve the feasibility and the safety of major complex hepatic resections. This study aims to review our experience in robot assisted major and extended hepatic resection.
Materials & Methods
We retrospectively reviewed data of all patients that underwent robotic assisted liver resections at two institutions by a single surgeon. From March 2002 to July 2009 a total of 76 robot-assisted hepatic resections were performed. Of those thirty (39.4%) were major hepatectomies including 22 right hepatectomy, 5 left hepatectomy and 3 right trisectionectomy with biliary reconstruction. There were sixteen man and fourteen women with a mean age of 57 years (range, 21-84 years).
Twenty patients (66.6%) had preoperative abdominal surgery. Eight resections (26.6%) were performed for benign tumors while twenty-two (73.3%) were performed for malignant tumors including liver metastases (sixteen patients), haepatoblastoma (one patient), HCC ( two patient), cholangiocarcinoma (three patients).
Results
All procedures were completed robotically but two (6,8%) that were converted because of bleeding. Nine patient had associate procedure including: main biliary duct resection with left hepaticojejunostomy ( 3), diaphragmatic resection ( 2), extensive adesyolysis ( 2 patients), colectomy( 1 patient), ventral hernia repair( 1). The mean operative time was 357 min (range, 220-660 min) with mean blood loss of 497 ml (range 240-2000 ml). No mortality occurred. Postoperative major morbidity occurred in four patients (13%).
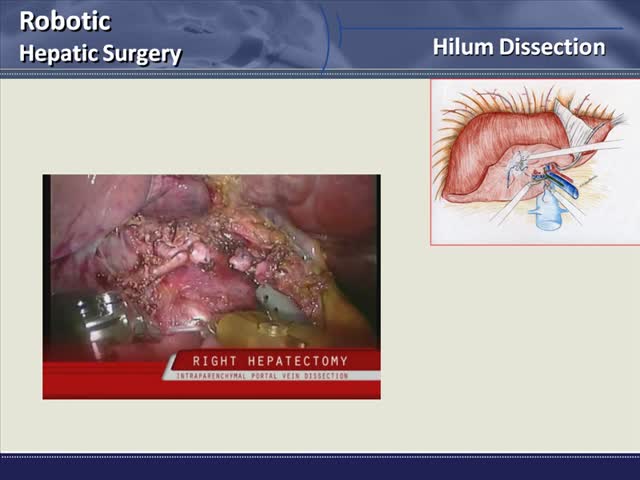
Conclusions
The results of this preliminary experience show that robot-assisted major and extended hepatic resections are feasible and safe. In this experience the rate of conversion is limited and postoperative morbidity is comparable to those of open surgery. Mainly two steps of the robot assisted procedure seem to be improved: the anatomical dissection of the hilum and the hepatocaval preparation with control of the accessories hepatic veins.
